OpenOvation · Thought Leadership in AI & Innovation
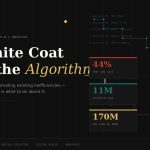
The White Coat Meets the Algorithm.
Most AI in healthcare right now is automating existing workflows — not transforming care. Understanding that distinction is the first advantage a healthcare professional can build in 2026.
S
Sudhir Shandilya
April 2026 · 18 min read
44%
Of healthcare workers fear AI will take their job
11M
Global healthcare worker shortage projected by 2030
50%
Drop in clinical documentation time expected by 2027
170M
New jobs projected globally from AI transformation by 2030
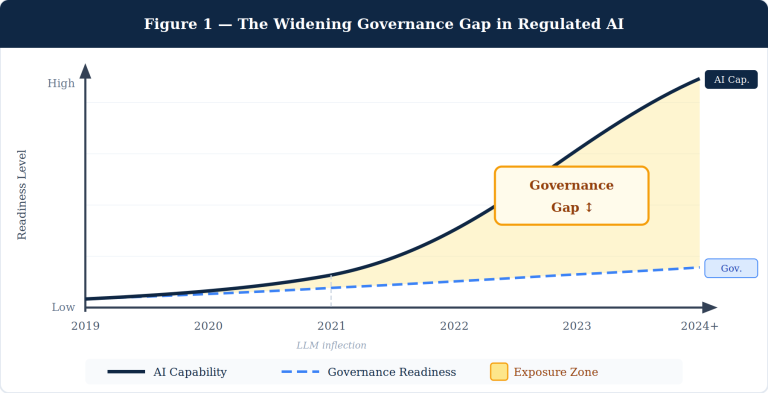
Here is the uncomfortable truth about AI in healthcare: most of what is being deployed right now is not transforming care. It is automating the inefficiencies that were already baked into broken workflows. Transcription automation does not redesign clinical documentation — it speeds up a process that should have been rethought years ago. Prior authorization bots do not fix a dysfunctional insurance system — they navigate it faster. That distinction matters enormously for how healthcare professionals should think about their position.
The anxiety is real and it is data-backed. Forty-four percent of healthcare workers fear AI will take their jobs — higher than the 35% cross-sector average. But fear tends to target the wrong thing. The greater risk is not replacement. It is that clinicians who do not understand AI well enough to evaluate it, challenge it, or shape it will progressively cede authority over decisions that directly affect their practice. Not their job titles. Their professional agency.
This article is structured as a practitioner’s guide, not a motivational overview. Five sections, each with a specific agenda: why the concern is legitimate, what to do about it now, what to learn and in what sequence, where the real opportunities are, and what students entering medicine today need to prioritize that the current curriculum does not yet require.
Section 01
The Concern Is Legitimate
What the data actually shows — and where the real displacement risk sits.
Acknowledge what is already happening. Medical transcription is 99% automated. Forty percent of medical coding is projected to be automated in 2025. Radiology technicians performing routine scans face documented displacement risk by 2030. These are not projections built on theoretical capability — they are production deployments in health systems operating today.
99%
Medical transcription already automated
DemandSage, 2025
40%
Medical coding projected automated in 2025
DemandSage, 2025
4.3%
Healthcare practitioners using GenAI for half+ their tasks — vs 19.2% in tech roles
SHRM Automation Survey, 2025
The Bureau of Labor Statistics’ 2025 AI impact analysis is clarifying on one point: no direct patient care roles made its list of AI-displaced occupations. The displacement risk is concentrated in healthcare-adjacent functions — coding, billing, administrative coordination, and roles built primarily on data retrieval and documentation. That is important context. It does not mean clinical roles are immune. It means the timeline and mechanism of impact is different.
For clinical roles, the more precise concern is what researchers call automation bias — the documented tendency for practitioners to defer to algorithmic outputs rather than interrogate them. FDA-cleared AI tools are already embedded in imaging workflows, clinical decision support systems, and EHR-integrated early warning alerts. When a clinician consistently accepts these outputs without critical evaluation, two things happen: patient risk accumulates silently, and the clinical judgment that took years to build begins to atrophy from disuse.
“I wonder if my years of training and expertise will be devalued by machines.”
— From qualitative research with healthcare workers on AI displacement concerns, SAGE Journals, 2024
That concern reflects a real dynamic — not because AI will devalue clinical expertise, but because healthcare systems will increasingly use AI outputs to justify staffing and scope decisions. The clinician who cannot articulate why an AI recommendation is wrong, or when a model’s training population does not resemble their patient panel, is operating at a structural disadvantage in those conversations.
The core risk is not job loss — it is loss of clinical authority. As AI-generated recommendations become standard in clinical workflows, the practitioner who cannot evaluate them critically will find their professional judgment progressively overridden by a system they do not understand.
The SHRM 2025 Automation Survey adds necessary precision: 63.3% of all jobs contain non-technical barriers that prevent complete automation — regulatory requirements, patient preferences for human contact, ethical accountability structures, and liability frameworks. Healthcare has more of these barriers than most industries. That is a structural protection. But it is not a reason to be passive. Those barriers will be eroded, negotiated, and worked around over time. The practitioners who understand that dynamic are the ones who will shape how it unfolds — rather than react to decisions already made.
Section 02
Five Moves to Make Right Now
Prioritized by impact, not ease — and sequenced for a practitioner with limited time.
The instinct to wait for institutional AI training programs is a mistake. Most health system AI education initiatives are a year or more behind the deployment curve. By the time your hospital offers a formal module on a tool, that tool will already be making decisions in your workflow. The practitioners who will have influence over how AI is implemented are the ones who built their understanding before the RFP was issued — not after the vendor contract was signed.
01
Build Your Conceptual Floor — This Week
Not a full course. A working vocabulary. Understand what a training dataset is and why its composition determines a model’s reliability. Know what “hallucination” means in a clinical AI context. Understand the difference between model accuracy on a validation dataset and model performance on your specific patient population. This knowledge costs you a weekend. Without it, you cannot meaningfully evaluate any AI tool that enters your practice.
02
Audit Your Workflow for Automation Exposure — Honestly
Categorize your daily tasks by type: pattern recognition, documentation, data retrieval, protocol navigation, patient-specific judgment, relational care, and ethical decision-making under ambiguity. The first three categories face near-term automation pressure. The last three do not — yet. This is not an exercise in anxiety. It is resource allocation: where should you be deepening expertise versus where are you investing energy in tasks that are likely to be automated within five years?
03
Get Into the Room Where AI Decisions Are Made
Health systems deploying AI pilots need clinical validators. If your institution is evaluating any AI tool — a documentation assistant, a predictive readmission model, a diagnostic support system — request to be part of the evaluation team. This is not additional workload. It is the most direct path to institutional influence over tools that will affect your practice. Clinical voices are systematically underrepresented in these procurement decisions. That absence has consequences.
04
Learn to Read a Clinical AI Validation Study
Vendors will cite AUC scores and sensitivity numbers without context. You need to know what to ask: On what population was this model trained? What were the demographic characteristics of the validation cohort? Has this been externally validated, or only on the development dataset? What is the false negative rate in underrepresented subgroups? These questions separate a clinician who can evaluate AI from one who accepts it. That distinction will define your professional authority in AI-integrated practice.
05
Commit to a Structured Learning Cadence — Not Passive Consumption
Thirty to sixty minutes per week, deliberately allocated. One peer-reviewed paper monthly from NEJM AI, The Lancet Digital Health, or npj Digital Medicine. FDA AI/ML updates when they publish. One professional society digital health committee, actively engaged. This is not optional professional development. In three to five years, AI fluency at this level will be an expected clinical competency in most specialties — not a differentiator.
🏥
Join Your Hospital’s AI Evaluation Committee
Clinical validators are scarce. Your participation shapes which tools get deployed, how they are configured, and what governance guardrails are required. This is direct influence — not overhead.
📚
Subscribe to NEJM AI
Launched in 2024, NEJM AI applies the same methodological rigor as the flagship journal to clinical AI research. Required reading for any practitioner who will evaluate AI tools in practice.
🎓
Complete One Structured AI Course
deeplearning.ai’s “AI for Medicine,” Stanford’s AI in Healthcare certificate, or MIT’s MedAI program — each completable in under eight weeks part-time and built specifically for clinical audiences.
📝
Engage Your Professional Society’s AI Guidelines
AMA, ANA, HIMSS, and specialty societies are actively writing AI practice standards. Clinicians who shape these guidelines now will determine what the rest of the profession is required to follow later.
The Evaluating Clinician. AI tools are already embedded in EHR workflows, imaging pipelines, and clinical decision support. The question is not whether clinicians will use them — it is whether they will use them with the critical judgment those tools require. · Photo: Unsplash
Section 03
What to Learn — In What Sequence
A tiered competency framework that builds AI fluency on top of clinical expertise — not in place of it.
The most common mistake healthcare professionals make when approaching AI upskilling is adopting the wrong reference frame. This is not a technology education problem. It is a clinical competency extension. You are not learning to build AI systems. You are learning to deploy, evaluate, and govern them within a professional context where the consequences of errors are measured in patient outcomes.
A 2025 systematic review in PMC examining AI skills for healthcare professionals identified three core domains: technical literacy, procedural competence in AI-assisted workflows, and the ethical and governance reasoning to know when AI recommendations should be overridden. The proportion of each domain required depends on role and specialty — but the foundational tier is universal.
Skill Domain
Tier
What to Learn
Why It Matters
AI Conceptual Literacy
All Clinicians
How ML models are trained, training data composition, confidence scores, hallucination risk in clinical outputs
You cannot evaluate tools you don’t understand. Non-negotiable baseline.
Critical Appraisal of AI Evidence
All Clinicians
Reading AI validation studies: AUC, sensitivity/specificity, external validation, subgroup performance
Vendors cite headline numbers. You need the questions that reveal where those numbers break down.
Clinical Decision Support Navigation
All Clinicians
AI recommendations as hypotheses to test, not conclusions to accept. Override protocols and documentation.
Automation bias is a patient safety issue already documented in live clinical systems.
Algorithmic Bias & Equity Reasoning
All Clinicians
How dataset bias translates to clinical inequity. Identifying when a model’s training population doesn’t match your patients.
Biased AI systematically underperforms for underserved populations — the exact patients where errors are most consequential.
Specialty AI Applications
Specialist Track
FDA-cleared AI tools in your specialty. Imaging AI, genomics decision support, medication optimization.
The specialist who knows which tools are validated, for whom, and under what conditions holds authority that others lack.
Health Data Governance
Specialist Track
HIPAA in AI contexts, de-identification standards, federated learning, patient consent for AI training data.
Patient trust is built or destroyed by how data is handled. This knowledge grants standing in governance decisions.
AI Procurement & Vendor Evaluation
Leadership Track
Vendor assessment frameworks, clinical validation requirements for procurement, implementation readiness.
CMOs and CMIOs who can’t evaluate AI vendor claims are making buy decisions on marketing materials. That’s a patient safety issue dressed as a procurement process.
AI Governance & Oversight Architecture
Leadership Track
Human-in-the-loop design, AI audit frameworks, FDA Digital Health Center, EU AI Act, CMS AI programs.
Deploying AI without governance creates accountability gaps that will surface as adverse events. Leaders who understand this prevent them.
One competency deserves emphasis beyond any table: the capacity for AI-independent clinical reasoning. As AI-generated recommendations become pervasive, the practitioner who retains the judgment to step outside them — to recognize when the model is wrong, when the presentation is atypical, when the patient in front of them defies the statistical pattern — becomes both rarer and more valuable. The deep clinical intuition built from years of direct patient contact is not obsolete in an AI environment. It is the primary check on AI error. Preserve it deliberately.
“Just as understanding Wi-Fi is necessary to navigate smartphones, clinicians must learn key concepts such as pretraining, embedding, and fine-tuning to use AI intelligently.”
— PMC / Perspectives on Medical Education, “Not Replaced, but Reinvented,” 2025
Section 04
Where the Real Opportunities Are
Emerging roles and pathways that require both clinical credentials and AI fluency — and where to find them.
The World Economic Forum projects 170 million new jobs globally by 2030, against 92 million displaced — a net positive of 78 million positions. Healthcare roles with AI augmentation are among the explicit growth drivers: nurse practitioners are projected to grow 52% from 2023 to 2033. The constraint is not that the opportunities do not exist. It is that most healthcare professionals are not positioned to compete for them because they have not built the complementary AI fluency those roles require.
Emerging Role
Clinical AI Validator
Health systems need clinicians who can evaluate model performance against real patient cohorts. This role doesn’t yet have a standardized title — early movers define what it looks like.
Emerging Role
Chief AI Medical Officer
An evolving C-suite designation at health systems and health tech companies. Still rare enough that practitioners building the right profile now will define the role rather than compete for it.
Emerging Role
Physician-Scientist, Medical AI
Academic medical centers are hiring dual-trained clinician-researchers to develop and validate AI tools. NIH’s NCATS and PCORI are funding this directly.
Emerging Role
Clinician Founder
The structural advantage of clinical domain expertise is one AI companies consistently fail to replicate by hiring non-clinical talent. The FDA’s Digital Health CoE actively supports clinician innovators.
Emerging Role
AI Ethics & Equity Advisor
Health systems and payers are creating roles for clinicians who can evaluate algorithmic equity implications. Rare, above-market compensation, and genuinely scarce supply.
Emerging Role
Clinical Informaticist
The operational bridge between clinical workflow and technical implementation. Knowledge of EHR architecture, FHIR, HL7, and clinical context is consistently in higher demand than supply.
Where to look — specific and actionable:
↗
Health Technology Companies
Verily, Tempus, Flatiron Health, Epic, Optum, and the clinical AI startup cohort are recruiting Medical Directors, Clinical Advisors, and VP-level roles requiring clinical credentials plus AI fluency. The differentiator in those searches is documented AI engagement — not credentials alone.
↗
Academic Medical Center AI Institutes
Stanford HAI, Johns Hopkins Malone Center, UCSF’s Bakar Institute, Mayo Clinic Platform, and Mass General Brigham’s AI program all hire clinicians into research and operational roles. Search within the specific institute, not the broader hospital system.
↗
FDA and CMS Regulatory Roles
The FDA’s Digital Health Center of Excellence is expanding its clinical review capacity. CMS is building AI capability for value-based care programs. Clinical credentials combined with regulatory understanding is a combination that is scarce and well-compensated when it exists.
↗
Thought Leadership as Career Infrastructure
A radiologist who publishes a substantive LinkedIn analysis of AI diagnostic tool limitations will attract more inbound opportunity than a CV update alone. Articulate clinical voices in AI are genuinely scarce. Writing, speaking, and contributing to public debate are hard differentiators — not soft career moves.
The Multidisciplinary AI Team. The most effective clinical AI deployments are led by practitioners who translate between the technical system and the patient care context. Engineers don’t have the clinical expertise. Most clinicians don’t yet have the technical fluency. That gap is the opportunity. · Photo: Unsplash
Section 05
For the Student Entering Medicine Now
You will complete training in 2030 or beyond. Here is what current accreditation standards will not prepare you for — and what you need to build yourself.
A 2025 PMC viewpoint on AI in medical education states it directly: most medical students currently lack understanding of the basic technical principles underlying AI, and medical education accreditation standards typically exclude AI competencies. That is a curriculum gap and a first-mover opportunity simultaneously. The student who self-educates on AI during training will enter residency with a competency that most attending physicians do not yet hold. That asymmetry is time-limited. Exploit it now.
The healthcare system you will enter at full clinical capacity — in the early 2030s — will have AI embedded in diagnostic workflows, treatment planning, discharge management, and potentially in surgical assistance. The question is not whether you will work alongside AI. It is whether you will understand it well enough to use it safely, challenge it when it is wrong, and shape how it is deployed in your practice environment.
For Pre-Med & Medical Students
Five Investments That Current Medical Curricula Will Not Make For You
These are not electives. They are the structural foundations of a clinical career that retains authority and relevance through the AI era — and the ones least likely to be handed to you by a standard medical education pathway.
1. Build real biostatistics and research methodology depth. Every AI tool you will evaluate in clinical practice is validated through a study. The clinician who can critically read that study — who understands AUC, sensitivity, specificity, NPV, subgroup performance gaps, and the implications of a homogenous training cohort — holds evaluative authority that algorithms cannot replicate. This is not statistical theory. It is clinical self-defense.
2. Get direct research experience in a medical AI lab during training. A summer in a clinical AI research environment at your institution, or an elective with research groups at Stanford HAI, Google Health, Microsoft Research Health AI, or a comparable academic center, is worth more than any certificate course. Being a practitioner who has actually been inside the development and validation process changes how you use and evaluate these tools for the rest of your career.
3. Develop the clinical competencies that AI cannot replicate — with the same rigor you bring to science. Communication under uncertainty. Ethical reasoning when the guidelines run out. The capacity to hold a patient’s values in view when clinical evidence is ambiguous. These are not soft skills — they are the irreplaceable core of clinical practice. Build them deliberately.
4. Choose your specialty with AI exposure clearly in your field of vision. Radiology, pathology, and genomics medicine are experiencing the most concentrated AI development — and will need the most AI-fluent clinicians to evaluate, govern, and safely deploy those tools. Do not avoid AI-exposed specialties out of displacement anxiety. Enter them with the AI literacy to lead rather than be led.
5. Build a professional intellectual presence now, not after residency. Write. Publish a perspective on a clinical AI paper you found important. Contribute to your institution’s AI working group or AMSA’s digital health chapter. The physician entering residency with a documented record of substantive AI engagement — not certificates, but actual thinking — is positioned for opportunities that the standard applicant pool cannot access.
Biostatistics & Research Methods Clinical Informatics Elective Medical AI Lab Research Health Equity & Algorithmic Bias EHR & Clinical Data Standards AI Ethics in Medicine Human Factors in Clinical Systems FDA Digital Health Regulation
The broader shift in medical education is a move from training physicians to memorize information toward training them to navigate, evaluate, and apply knowledge in context. AI can surface the current treatment protocol faster than any clinician can recall it. What AI cannot do is determine whether that protocol applies to this patient — with this comorbidity profile, in this social context, with these stated preferences and values. That contextual, patient-specific judgment is the core of clinical practice. Students who understand that are preparing for the right job.
“The clinician who fears AI is asking the right question. The one who stops there is making the wrong decision. The question that matters is not whether AI will change your practice — it will. The question is whether you will understand it well enough to shape how.”
— Sudhir · OpenOvation
References & Sources
01TempDev. (2025). 65 Key AI in Healthcare Statistics.tempdev.com
02DemandSage. (2026). 77 AI Job Replacement Statistics 2026.demandsage.com
03SHRM. (2025). Automation, Generative AI, and Job Displacement Risk in U.S. Employment.shrm.org
04National University. (2026). 59 AI Job Statistics: Future of U.S. Jobs.nu.edu
05World Health Organization. (2023). Health Workforce Projections 2030. Geneva: WHO.
06Rony, M.K.K., et al. (2024). Concerns About the Replacement of Medical Professionals by AI. SAGE Open Nursing. doi:10.1177/23779608241245220
07PMC / Perspectives on Medical Education. (2025). Not Replaced, but Reinvented.pmc.ncbi.nlm.nih.gov
08eClinicalMedicine / The Lancet. (2025). AI Education for Clinicians.thelancet.com
09Frontiers in Education. (2025). Integrating AI into Pre-Clinical Medical Education.frontiersin.org
10PMC. (2025). AI in the Health Sector: Systematic Review of Key Skills.pmc.ncbi.nlm.nih.gov
11The Lancet Digital Health. (2025). How Can AI Transform Medical Student and Physician Training?thelancet.com
12OECD. (2025). Digital and AI Skills in Health Occupations. Working Paper No. 36. oecd.org
13World Economic Forum. (2025). Future of Jobs Report 2025. Geneva: WEF.
14Bureau of Labor Statistics. (2025). AI Impacts in BLS Employment Projections.bls.gov
15HIMSS. (2024). The Impact of AI on the Healthcare Workforce. Chicago: HIMSS.
16WHO / PMC. (2020). AI: Opportunities and Implications for the Health Workforce.pmc.ncbi.nlm.nih.gov