And the design fix is not a better EHR. It is a governed agentic AI architecture.
• • •
Working memory holds three to five items at a time. That is not an estimate. That is a hard biological constraint. When you exceed it, performance does not just slow — it degrades. Judgment deteriorates. Pattern recognition fails. Shortcuts replace reasoning.
This is Cognitive Load Theory, formulated by John Sweller in 1988. It is not controversial. It is foundational cognitive science.
Now consider the environment we have built for clinicians: hundreds of lab values per patient, drug interactions to verify in real time, EHR screens designed by engineers rather than clinicians, hundreds of alert notifications per shift, documentation requirements extending into personal hours, prior authorization requests stacking up in the background, and administrative overhead consuming nearly two clinical days per week per physician.
We are running a system that structurally exceeds the cognitive limits of the people it depends on. And then we wonder why errors happen.
This is not a wellness problem. Resilience training and mindfulness programs do not change the architecture. They ask individuals to adapt to a system that is broken at the design level. That is the wrong intervention.
The right intervention is redesigning how cognitive work flows — what humans carry, what systems carry, and where accountability lives. That is what governed agentic AI makes possible. And that is what this article is about.
I. What Cognitive Overload Actually Means in Healthcare
Three types of load operate simultaneously in any clinical encounter.
Intrinsic load is the inherent complexity of the task. A patient with 14 comorbidities, polypharmacy risks, ambiguous imaging, and a complicated social history. This load cannot be eliminated. It is medicine.
Extraneous load is the cognitive friction added by poor system design — fragmented EHR interfaces, redundant data entry, clinically irrelevant alerts, disconnected systems that force constant context-switching. This load is entirely manufactured by infrastructure failure. It is avoidable.
Germane load is the productive work of clinical reasoning — updating a diagnosis, revising a care plan, integrating new evidence. This is what clinicians trained for. But when intrinsic and extraneous loads are already maxed out, there is no bandwidth left for germane processing. Heuristic shortcuts take over. That is when errors happen.
The tragedy of EHR adoption is that it was designed to help and has instead dramatically increased extraneous load. Research published in JMIR Medical Informatics in 2024 concluded that inadequate presentation of large volumes of clinical data, combined with complex interfaces, adds cognitive work rather than reducing it. EHRs have become one of the primary drivers of the very burnout they were meant to prevent.
II. The Data Is Not Ambiguous
On burnout: The AMA’s 2024 National Physician Burnout Study found 43.2% of physicians reporting at least one burnout symptom. Down from the pandemic peak of 62.8%, but nearly half the workforce remains in a state of chronic exhaustion. A Stanford Medicine-led study published in April 2025 confirmed this — and their chief wellness officer made the consequence explicit: burnout correlates directly with physicians leaving the profession and reducing clinical hours, at the exact moment healthcare faces severe workforce shortages. Emergency medicine physicians lead at 68% emotional fatigue. Therapists report the highest mental fatigue (77%) and the highest cognitive impairment of any specialty (39%).
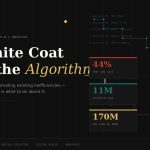
On documentation: Primary care physicians spend approximately three hours per day on clinical documentation alone. When all administrative requirements are included, the AMA estimates physicians would need 27 hours per day to complete everything. “Pajama time” — after-hours documentation bleeding into personal life — is so normalized it has its own clinical term. The U.S. Surgeon General-endorsed 25×5 Initiative aimed to reduce documentation burden by 75% by 2025. Progress has been marginal.
On administrative overhead: Physicians spend an average of 15.6 hours per week on administrative work — nearly two full clinical days per week lost to non-clinical tasks. The prior authorization process alone accounts for a median of 43 requests weekly, consuming approximately 12 staff hours. Nine in ten physicians say PA negatively affects patient outcomes. Nearly one in four report that a patient in their care suffered a serious adverse event — hospitalization, permanent impairment, or death — because treatment was delayed.
On decision fatigue: A 2025 systematic review synthesizing 82 studies found clear evidence of decision quality degradation over a healthcare professional’s shift. Residents described it as “perceived cognitive dysfunction” — slowed processing, working memory deficits, impaired executive function. The probability of high-value clinical decisions decreases as the day progresses. Low-value decisions increase.
On errors: Each interruption during drug preparation raises error probability by 25%, because the nurse must restart the cognitive sequence from zero. A one-unit increase in alarm fatigue among ICU nurses correlates with a 0.381 increase in tendency toward medical errors. Sleep-related impairment in physicians directly associates with higher rates of clinically significant errors.
This is not anecdotal. This is a documented system failure with measurable consequences for patients.
III. The 18 Places Cognitive Overload Shows Up
Cognitive overload is not a single clinical phenomenon. It runs across every role and every function in healthcare. Understanding where it lives is prerequisite to designing systems that address it.
Clinical Settings
1. ICU and Critical Care — The Alarm Problem
Almost all ICU nurses experience high cognitive load. Research is unambiguous on this. The mechanism is alarm fatigue — a phenomenon where repeated exposure to frequent, mostly non-actionable alarms leads to sensory overload, desensitization, and reduced responsiveness. A 2025 qualitative study across three teaching hospitals found that alarm fatigue develops through three states: cognitive reserve deficit, load balance, and overload — with overload as the immediate trigger for dangerous behavior. Nurses describe near-miss events where silencing an alarm out of accumulated fatigue almost cost a patient’s life when a genuine crisis emerged moments later. Selective inattention becomes a rational response with irrational consequences.
2. Emergency Medicine — Speed and Load Collide
Emergency physicians manage multiple patients simultaneously across the full acuity spectrum — interpreting evolving diagnostics, coordinating teams, documenting in real time, making high-stakes decisions under time pressure. Decision fatigue accumulates rapidly. Triage quality, analgesic prescribing accuracy, and diagnostic ordering reliability all degrade demonstrably over a long shift. The brain does not multitask. It switches contexts. Each switch carries a cognitive cost. In emergency medicine, that cost is measured in seconds.
3. Radiology — Volume Versus Vigilance
Radiologists read hundreds of images per shift. Volume-based productivity metrics — reads per hour — create structural incentives for speed that directly conflict with the attentional demands of catching rare, consequential findings. Cognitive tunneling is documented: focused attention on one finding can cause perceptual misses of co-occurring pathology. The AHRQ has explicitly stated that high cognitive load likely impacts diagnostic accuracy and that the radiologist’s cognitive environment needs systematic redesign.
4. Surgery — Precision Under Accumulation
Surgeons in the OR manage procedural execution, anesthesia coordination, patient monitoring, unexpected intraoperative findings, and team communication simultaneously. Research in surgical ICU settings shows that continuous alarm exposure combined with high-precision care demands generates cognitive overload that directly affects performance accuracy and care quality.
5. Primary Care — The Impossibility of Full Scope
The math does not work. Thirty patients per day, each with unique chronic disease profiles, preventive care gaps, medication reconciliation needs, and social determinants to address — in fifteen-to-twenty-minute windows. The result is systematic triage — not of patient urgency, but of cognitive bandwidth. What gets skipped is not random. It is what the system has no capacity to hold.
6. Oncology — The Knowledge Gap
Medical knowledge in oncology doubles approximately every 73 days, per NIH estimates. No clinician, however skilled, can maintain current knowledge across genomics, imaging, pathology, drug interactions, clinical trial eligibility, and patient-specific comorbidities — while also delivering active care. The gap between available evidence and applied clinical reasoning in oncology is not a training failure. It is a cognitive capacity failure.
7. Pharmacy — The Alert Override Problem
Clinical pharmacists in high-volume settings review hundreds of prescriptions per shift for drug interactions, dosing errors, contraindications, and allergy conflicts. Alert override rates in pharmacy systems are widely documented and high. When every click generates a warning, warnings lose signal value. Pharmacists learn — rationally, dangerously — to override alerts rapidly to maintain throughput. Safety margin is traded for workflow survival.
8. Nursing — The Multidimensional Load
Bedside nurses carry perhaps the most distributed cognitive burden in healthcare. Patient monitoring, medication administration, care coordination, documentation, patient education, family communication, and rapid response to deterioration — simultaneously, continuously. Missed nursing care — tasks intended but not completed — is a documented consequence of cognitive overload. These are not individual failures. They are system design failures.
9. Telehealth — Context Without Continuity
Telehealth clinicians must build a diagnostic picture without physical examination, from patient-reported data and limited visual cues, across back-to-back appointments with no transition time. Records are fragmented across platforms. Information continuity that should be structurally provided must be mentally reconstructed by the clinician — every encounter, every patient.
10. Behavioral Health — When Emotional Labor Meets Cognitive Depletion
Therapists and psychiatrists experience a compounding dynamic that most system designs ignore entirely. The 2025 Tebra research found therapists reporting the highest mental and physical fatigue of any specialty, the highest loss of motivation, and the highest cognitive impairment rate (39%). Compassion fatigue and cognitive overload do not exist as separate phenomena in behavioral health. They reinforce each other in a cycle that current systems do nothing to interrupt.
Operational Settings
11. Prior Authorization — Non-Clinical Work Consuming Clinical Bandwidth
The cognitive cost of prior authorization is not just volume. It is rule complexity. Each payer maintains different, shifting approval criteria. Managing 15 payers’ simultaneous rule sets depletes the same working memory that clinical reasoning requires. McKinsey analysis showed that automating the PA process — redirecting half the RN time currently consumed by it — would be equivalent to adding over 100,000 nurses to the workforce. This is not an efficiency metric. It is a structural reallocation of cognitive capacity currently being consumed by bureaucracy.
12. Revenue Cycle Management — Error Amplification Under Pressure
RCM teams operating under volume pressure and denial backlogs face compounding error risk. Medicare Advantage denial rates rose 4.8% from 2023 to 2024. Each denial triggers a review, appeal, and resubmission cycle downstream of an initial error that was often a documentation shortcut made upstream under load. The chain reaction from a single cognitive failure under pressure can extend weeks and write off thousands of dollars.
13. Compliance and Quality Reporting — The Regulatory Complexity Stack
Compliance officers maintaining working knowledge across HIPAA, CMS requirements, Joint Commission standards, ONC mandates, and evolving state-level regulations — while managing daily operations — are operating at sustained cognitive load. Regulatory surface area is expanding faster than human capacity to track it manually.
14. Care Coordination at Transitions
Care coordinators managing patient transitions between acute, post-acute, and outpatient settings are working across information asymmetries that should be handled by systems but are instead carried in human working memory. What the hospital knows versus what the skilled nursing facility knows versus what the primary care physician knows — that gap is bridged manually, cognitively, at the coordinator’s expense. These are cognitive load failures.
15. Infection Control and Surveillance
Infection preventionists monitoring for hospital-acquired infections, antibiotic stewardship compliance, and outbreak signals are working against data volumes that exceed manual analysis capacity. The data exists. The capacity to act on it in real time does not.
16. Patient Safety Reporting
Risk management teams reviewing incident reports must categorize events, conduct root-cause analysis, identify systemic patterns, and track remediation — across high volumes, continuously. When volume exceeds analytical capacity, safety signals go unanalyzed. Near-misses are closed without learning. System improvements that could prevent future harm are never initiated because the cognitive work required to connect pattern to action is unavailable.
17. Supply Chain and Resource Management
Healthcare supply chain management under manual cognitive models is fundamentally mismatched to the dynamic, multi-variable reality of healthcare operations. The COVID-19 pandemic made visible how catastrophically this fails at scale. The failure mode is not data absence. It is cognitive processing capacity that cannot act on available signals in real time.
18. Clinical Trial Coordination
Research coordinators managing protocol compliance, enrollment, data collection, and regulatory submission across multiple concurrent trials operate under extraordinary cognitive demand. Protocol deviations cited in FDA inspection findings frequently trace to documentation errors made under load during high-enrollment periods. Precision is the job. The conditions are designed against it.
IV. Why Conventional Interventions Have Not Worked
The existing playbook has three categories: system improvements, training, and wellness. All three fail at the same point.
EHR optimization improves interfaces without eliminating underlying burden. Training builds individual resilience without reducing systemic demand. Wellness programs — mindfulness, coaching, scheduled breaks — treat symptoms while the load continues to accumulate.
Every conventional solution operates at the level of the individual. It asks the clinician or the administrator to adapt, absorb, and cope. It does not restructure the information environment. It does not reduce the number of decisions a human must make. It does not eliminate extraneous load.
In systems thinking, this is intervening at the symptom rather than the leverage point. The leverage point is workflow architecture. And restructuring workflow architecture requires a different category of tool.
V. Agentic AI: The Structural Answer
Agentic AI is not a smarter autocomplete. It is a goal-directed autonomous system that can decompose complex objectives, coordinate specialized agents across disparate data sources, execute multi-step tasks, and adapt based on outcomes — within defined human oversight structures.
The distinction from traditional AI is operationally significant. Traditional decision support adds one more data point to an already overloaded screen. Agentic AI reduces the number of decisions a human needs to make, routes the right information to the right person at the right moment, and executes non-clinical tasks autonomously — preserving cognitive capacity for work that genuinely requires human judgment.
The evidence is building. Research published in Frontiers in Artificial Intelligence found agentic architectures can reduce cognitive workload by up to 52% compared to traditional clinical decision support. A 2025 ICU framework validation demonstrated 45% cognitive load reduction alongside a 30% mortality reduction and 85% improvement in sepsis bundle compliance. McKinsey’s 2024 healthcare AI analysis found organizations implementing agentic AI reporting 40–60% reduction in administrative costs and 25–35% improvement in diagnostic accuracy. These are not marginal gains.
Where agentic AI directly addresses the use cases above:
- Ambient clinical documentation — Agentic systems record, structure, and summarize patient encounters in real time, eliminating the three-plus daily hours of documentation burden. The next evolution is EHR action — pulling vitals, flagging follow-ups, updating care plans, all from voice-directed commands. As one chief medical officer put it plainly: “I didn’t go to medical school to be a scribe.”
- Intelligent alarm triage — Rather than delivering every alarm simultaneously, agentic systems evaluate clinical relevance in real time, suppress non-actionable alerts, escalate genuinely critical signals, and deliver a single prioritized notification. This directly targets the alarm fatigue mechanism driving error rates in ICU settings.
- Prior authorization automation — Agentic PA systems assemble payer-specific documentation, submit across multiple channels, monitor authorization status, and generate appeal letters with supporting evidence — removing the 12 staff hours per physician per week currently consumed by this process.
- Diagnostic synthesis for complex cases — Multi-agent architectures operating as virtual multidisciplinary teams — specialized agents for clinical notes, genomics, biochemical markers, imaging, and pathology — can synthesize information at a scale and speed no single clinician can match under active care demands.
- Care transition coordination — Proactive monitoring of patients moving between settings, automatic identification of information asymmetries, triggered communication to receiving providers, medication reconciliation risk flagging, and follow-up scheduling — converting reactive coordination into anticipated action.
- Predictive deterioration monitoring — Continuous monitoring for subtle physiological changes, with automated alerts before clinical thresholds are crossed. This shifts the clinical posture from reactive response to anticipated intervention — fundamentally lower cognitive load.
- Revenue cycle intelligence — Real-time eligibility verification, predictive denial modeling, automated claims submission, and self-correcting appeal management — transforming a cognitively taxing reactive process into an autonomous workflow.
- Regulatory compliance automation — Continuous documentation monitoring against regulatory requirements, proactive gap flagging, and real-time tracking of evolving payer rules — eliminating the cognitive tax of manual regulatory surveillance.
The throughline is consistent: agentic AI absorbs the extraneous load and returns cognitive space for the intrinsic load. That is the trade that matters.
VI. Capability Without Governance Is Not a Solution
Here is where most of the current conversation stops. It should not.
Deploying agentic AI in healthcare without structured governance is not relief. It is risk transfer. The same autonomous capability that reduces cognitive load can generate catastrophic outcomes if it operates outside defined accountability structures.
When an agentic system incorrectly suppresses a clinical alarm, the consequence is patient harm. When it makes a documentation choice that misrepresents a patient’s condition, the consequence is regulatory exposure. When it submits a PA request that does not accurately reflect medical necessity, the consequence is institutional liability. None of these failure modes are theoretical. They are the predictable outcomes of capability deployed without governance.
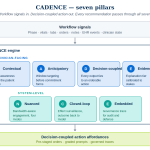
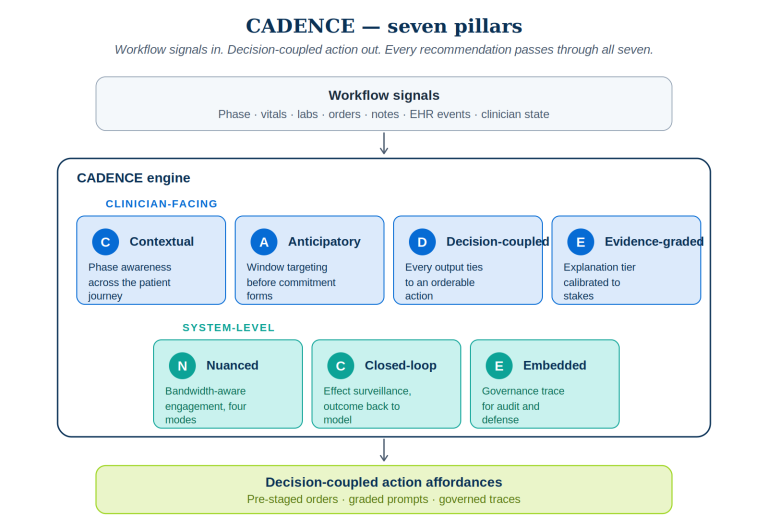
This is the problem that PRAXIGOV was designed to address.
PRAXIGOV is a multi-stage governed pipeline for agentic AI workflows in regulated industries. It does not bolt governance on as a monitoring layer after deployment. It builds governance into the workflow architecture from intake through output — so that every agentic action is traceable, every decision boundary is explicit, and every escalation path is defined before a single agent executes a task.
Examined through the PRAXIGOV lens, the cognitive overload problem is reframed. The question is not “how do we automate more?” It is “how do we govern agentic action so that automation can be trusted?” In regulated industries, that is the more important question.
Intake before architecture. Any agentic system addressing cognitive load in healthcare must begin with precise domain anchoring — the specific patient population, the specific regulatory context, the specific risk tolerances of the institution. Upstream precision prevents downstream errors that governance cannot retroactively correct.
Accountability at every decision node. Every action an agentic system takes in a clinical or operational workflow must be tied to an accountable human role — not as a formality, but as the mechanism that makes oversight real. Distributed accountability is not the enemy of automation. It is its prerequisite.
Explicit autonomy boundaries. Agentic systems in healthcare must have pre-defined boundaries specifying what the agent decides autonomously, what requires human review, and what requires human approval. These boundaries are not static configurations. They are living governance structures that reflect current reviewer capacity, the risk profile of the decision domain, and the agent’s performance track record.
Schema consistency across the workflow. One of the most insidious failure modes in multi-agent systems is field drift — where the data schema used by one agent is subtly different from what the next agent expects, generating downstream errors that are difficult to trace and clinically consequential. Cross-stage schema validation is not an engineering preference. In clinical settings, it is a patient safety requirement.
Simulation before production. Deploying an agentic system into live clinical workflows without rigorous governance simulation is not acceptable in a regulated environment. Testing must cover escalation pathways, boundary conditions, edge cases, and failure modes — including understaffed shifts and high-volume periods — before any autonomous action reaches a patient or a payer.
Governance trace for every output. Every output of a governed agentic workflow must carry a traceable audit log — for regulatory compliance, yes, but more fundamentally for continuous learning and accountability. The output layer is not the end of the workflow. It is the beginning of the accountability record.
The capacity-aware dimension — the hardest part to get right.
Human reviewer capacity is a dynamic variable. It changes by shift, by staffing level, by patient census, by time of day. A governance framework that ignores this treats an 8 AM fully staffed clinic the same as a 3 AM understaffed unit. They are not the same. Agentic autonomy should flex with the institutional capacity to oversee it — in real time.
This is the core of the PRAXIGOV capacity-aware throttle: AI output should be modulated based on the actual, real-time capacity of human reviewers to govern what the system produces. The same agentic action that is appropriate when six reviewers are available may be inappropriate when one is. That dynamic is not an implementation detail. It is a governance imperative.
Healthcare leaders designing agentic AI programs must hold three questions simultaneously:
- What can the AI do?
- What should the AI do?
- What should the AI do given who is available to review it right now?
Most programs answer only the first. The third question is where patient safety lives.
VII. What This Requires of Healthcare Leaders
Cognitive overload in healthcare is structural. It will not resolve through individual adaptation or incremental system optimization. It requires a redesign of how cognitive work is distributed across humans and systems — and it requires governance architecture that makes agentic action trustworthy before it is scaled.
The organizations that will lead in the agentic era are not those that deploy the most agents fastest. They are those that build the governance infrastructure first — so that when autonomous systems act, they act within boundaries that are explicit, accountable, and auditable.
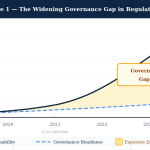
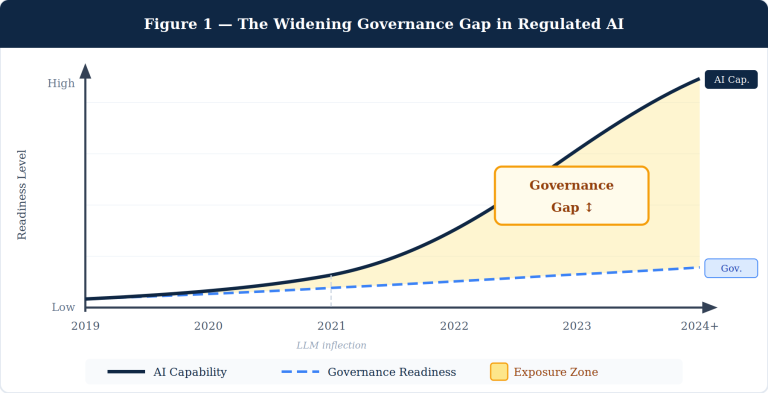
The evidence on cognitive overload is unambiguous. The evidence for agentic AI’s structural relief potential is compelling and growing. The governance gap is real, documented, and consequential.
The question facing every healthcare leader, clinical informaticist, AI strategist, and governance architect right now is not whether to build governed agentic systems. It is whether the governance architecture gets built before or after the first preventable harm occurs from an ungoverned one.
That choice is being made right now. In every health system. Every day.
The frameworks to make it correctly already exist.
Research in this article draws from: JMIR Medical Informatics (2024), AMA National Physician Burnout Study (2024), Stanford Medicine (2025), Frontiers in Public Health (2025), Agency for Healthcare Research and Quality, Tandfonline Systematic Review on Decision Fatigue (2025), GE HealthCare Research, MIT Technology Review, McKinsey & Company Healthcare AI Analysis (2024), IAPP, Harvard Edmond & Lily Safra Center for Ethics, npj Digital Medicine, and Tebra Healthcare Burnout Research (2025).